A new research paper in pre-print circulation at the open access journal Medical & Clinical Research raises the horrifying possibility that certain Covid-19 patients were euthanized during the pandemic.
The research paper has not been peer-reviewed; but it does provide data and documentation that is leading to pointed accusations directed at the National Heath Service (NHS) in the United Kingdom that doctors pursued a deliberate policy of euthanizing certain Covid-19 patients, particularly those patients struggling with pulmonary-respiratory issues.
Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19 Pandemic explores the stark lagged correlation between patient injections of the palliative sedative midazolam in certain regions of the United Kingdom and Covid-19 excess mortality rates.
The most striking dataset compares the monthly U.K. England excess deaths with monthly midazolam injections. Reported excess deaths follow upon injections by one month.
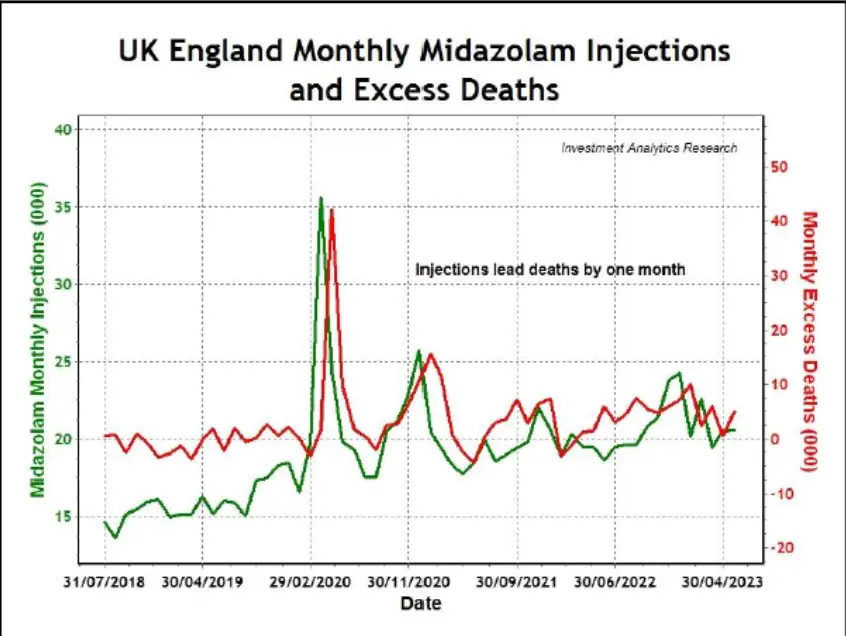
“Clearly, Midazolam injections and excess deaths in England are highly correlated, but not synchronously, because medication generally does not have instantaneous impact and also reporting of dosages used and registration of deaths may lag,” the author Wilson Sy of Investment Analytics notes. “Shifting the time series for Midazolam injections one-month forward, very high correlation is seen in Figure 10.”
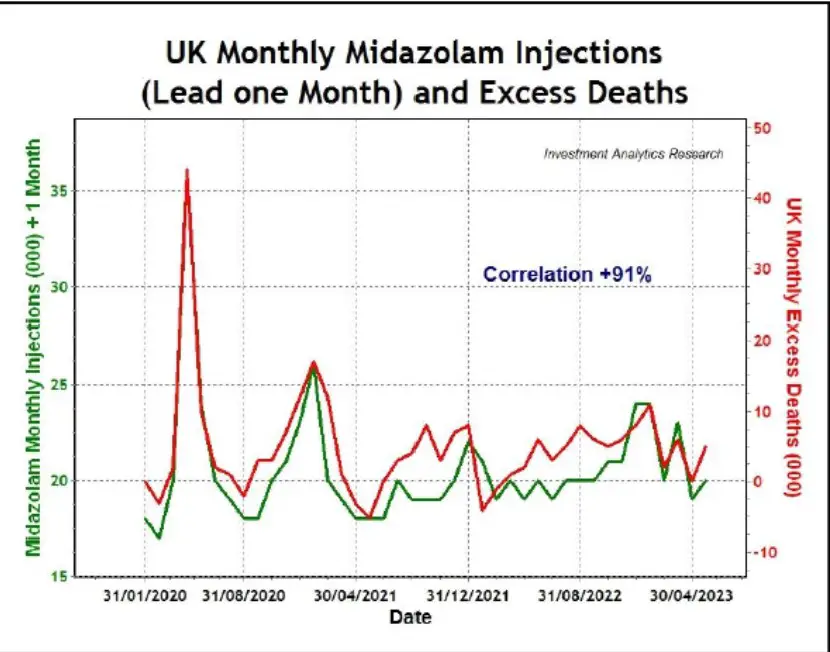
“The very high correlation (coefficient 91 percent) between excess deaths lagged one month after Midazolam injections is largely due to the first two enormous spikes to early 2021. From April 2021 onwards to May 2023, the same correlation dropped to 59 percent, but still statistically significant with p-value at 0.0007. The misclassification of COVID deaths, possibly deliberate, also led to their high correlation with Midazolam injections as seen Figure 11,” the author adds.
The author critically notes that the U.K. health service opened up the potential of abuse of palliative care policies for Covid-19 patients.
New guidelines were rapidly developed in early 2020 by the National Institute for Health and Care Excellence (NICE) for managing COVID-19 symptoms, including those at the end-of-life [22]. The rapidly developed new guidelines effectively opened the door to implement a policy of euthanasia in UK during the pandemic: “NICE has developed these recommendations in direct response to the rapidly evolving situation and so could not follow the standard process for guidance development. The guideline has been developed using the interim process and methods for developing rapid guidelines on COVID-19.
The pharmacological measures for managing breathlessness during the Covid-19 outbreak included the administration of morphine and midazolam.

- Opioid: Morphine sulfate 10 mg over 24 hours via a syringe driver, increasing stepwise to morphine sulfate 30 mg over 24 hours as required.
- Benzodiazepine if required in addition to opioid: Midazolam 10 mg over 24 hours via the syringe driver, increasing stepwise to midazolam 60 mg over 24 hours as required.
Morphine and midazolam as a tandem drug therapy has been controversial due to reports of abuse for palliative care and for lethal injections of convicted felons.
For example, during Hurricane Katrina in the United States in 2005, Dr. Anna Maria Pou, a cancer surgeon on the faculty of Louisiana State University School of Medicine, was accused of abusing morphine and midazolam to euthanize patients. At least 34 patients died at Memorial Medical Center under suspect conditions; however, a grand jury refused to indict Dr. Pou and four of her medical colleagues, the New England Journal of Medicine reported.
In 2022, the New York Times reported on the use of midazolam for lethal injections of prisoners.
The first full trial on Oklahoma’s use of midazolam played out this week, in a state where a prisoner vomited and shook for several minutes after he was injected with the sedative during an October execution. In the case before Judge Stephen P. Friot of the U.S. District Court in Oklahoma City, a group of prisoners on death row argued that the mix of drugs that awaits them in that state has the potential to cause so much pain as to be “constitutionally intolerable.”
The U.S. Supreme Court allowed the use of midazolam in a 2015 ruling in the same Oklahoma case, but the current trial has allowed for additional expert testimony and presentations of detailed research about the real-world use of the drug in execution chambers.
The Mayo Clinic has probed the ethics of administering midazolam for end-of-life care and explains its popularity and prevalence in palliative treatment.
Most centers use a midazolam-based regimen for PS because of the drug’s short half-life, relatively benign adverse effects, ease of intravenous or subcutaneous administration, and generally good efficacy.5,9–11 Other programs that use primarily barbiturates, either alone or in combination with other agents, have also reported good results.12–14 Our institution (Mayo Clinic, Rochester, MN) supports the use of ketamine or propofol in patients whose condition is refractory to opioids and midazolam.
Importantly, the author of the new research paper attempts to draw on statistical regional analysis of the United Kingdom to further elucidate whether correlations are a ghost of understandable hospital practices during a pandemic; a reflection of widespread Covid-19 vaccinations; or played an underlying causal role in excess mortality rates.
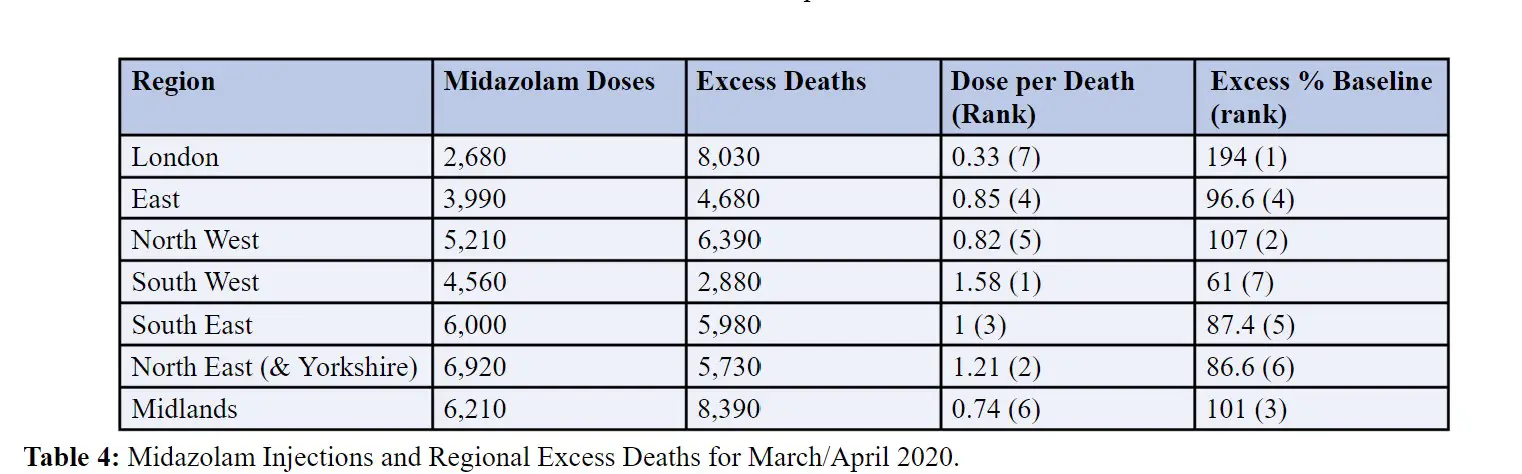
“Note that all regional subpopulations have consistently positive correlations, avoiding Simpson’s Paradox and suggesting the absence of signicant confounding factors in the statistical relationships. That is, even though the mathematical details of the regressions may differ quantitatively (due to other minor confounding factors), the firm conclusion prevails that Midazolam injections have significant causal impact on excess deaths in England,” Sy claims.
But the critical question is raised whether the use of midazolam overlapped entirely with patients who were bound to die regardless or whether the drug played a causal factor in producing more deaths.
“About 28,000 care home residents died in April 2020 across England, which represented about one third or 33.5 percent of all deaths in England. As there were about 375,000 care home residents (three quarters elderly, some with dementia, and the rest disabled) in an English population of 65 million, the mortality rates for that month were 7.5 percent and 0.128 percent respectively, implying an April 2020 death rate in care homes about sixty times (X60) that of the national average.,” Sy adds. “Many of the UK elderly with comorbidities or terminal illnesses have died with euthanasia in care homes, and not from COVID-19 due to few cases of infections early in 2020.”
This provocative claim is a challenge to the widespread conclusion that Covid-19 was of particular lethality to the elderly population. Sy, however, is attempting to raise the issue of medical malpractice and unethical guidelines, such as the abuse of palliative care and blanket Do Not Resuscitate (DNR) orders as exacerbating factors that contributed to drive up Covid death rates.
The research paper then attempts to tease out by comparison between U.K. England and Australia whether vaccination or euthanasia are major contributing factors to high excess mortality rates, particularly in the absence of a viral pandemic that has become endemic, since the majority of human beings have acquired immunity.
The research paper thus raises alarming questions that provoked a former Member of Parliament to ask if this was the “crime of the century.”
THE CRIME OF THE CENTURY : THE MIDAZOLAM MURDERS
If the data is correct, the only conclusion is that tens of thousands of elderly English were murdered with an injection of the end of life drug Midazolam.
These deaths were then falsely blamed on Covid, which was the basis of… pic.twitter.com/hGud7b1V1G
— Craig Kelly (@CKellyUAP) February 10, 2024
“If the data is correct, the only conclusion is that tens of thousands of elderly English were murdered with an injection of the end of life drug Midazolam,” remarked former MP Craig Kelly. “These deaths were then falsely blamed on Covid, which was the basis of the public fear campaigns used to justify the lockdowns and mass mandated injections of the public (including children) with an experimental medical intervention that had zero long term safety data. And along the way, a small group pushing the need for mass mandated injections made billions.”
This is certainly a premature assessment of the role of midzolam in exacerbating high excess mortality rates during and after the Covid pandemic. However, the research is suggestive of the role that alleged hospital malpractice — including the use of respirators, blanket DNR orders, social isolation, drugs like remdesevir, and abuse of palliative drugs like midzolam — played a major role in driving up excess mortality rates, in addition to questions about data malfeasance and fraud, and of course, Covid vaccines.
NOW READ:








{kind=link}